It’s with mixed emotions as we bid farewell to our lab head, Prof Allison McKendrick. She will be taking on the position of inaugural Lions Eye Institute UWA Chair in Optometry Research at The Lions Eye Institute and The University of Western Australia from November 2022.
Prior to her departure, we organised a surprise lab retreat to Portarlington and it was such a success! Allison was left speechless for minutes when she realised that it wasn’t a coincidence but rather a thoroughly prepared surprise for her! It was a relaxed one night trip that gave us a precious opportunity to catch up on all the happenings in life outside of work.
The Department of Optometry and Vision Sciences also organised a warm farewell afternoon tea to reminisce on the great achievement and contributions Allison has gained and input to optometry and science over the past 17 years.
Allison & Andrews: from left Andrew Anderson, Andrew Metha, Allison McKendrick, Andrew Turpin, Andrew Huhtunen
This also marks the end of the Clinical Psychophysics Unit laboratory at the Department of Optometry & Vision Sciences, The University of Melbourne. We would like to express an enormous thank you to all individuals who have contributed to our research: our valued research participants, visiting researchers, staff and students.
Allison’s new contact details are: allison.mckendrick@uwa.edu.au or allison.mckendrick@lei.org.au
The past July was a happy month for our lab member Juan Sepulveda and his supervisors, as his thesis named “Central and peripheral motion perception in healthy ageing and its potential relationship with driving” passed the examination to obtain the PhD degree. Juan’s thesis was supervised by Prof. Allison McKendrick and A. Prof. Andrew Anderson from the Department of Optometry and Vision Sciences at The University of Melbourne, and Prof. Joanne Wood from the Centre for Vision and Eye Research, School of Optometry and Vision Science at Queensland University of Technology.
Juan and his supervisors celebrating with Chilean wine (8 pm in Chile), and Australian roasted coffee (10 am in Australia)
In his thesis, Juan explored what happens to the perception of visual motion in older adults. Juan assessed performance for a range of different moving stimuli, and considered situations of relevance to driving (i.e. simulating nighttime driving and driving under the presence of car headlights), finding that the deficits experienced by older adults were mostly related to difficulties detecting low contrast patterns. Additionally, Juan found a mild relationship between motion perception tests and a commonly used video-based test of driving, the Hazard Perception Test. Juan recently presented these findings at the 2021 European Conference on Visual Perception (ECVP). The Hazard Perception Test is used in many jurisdictions to apply for a driver’s license. It measures the ability to identify and predict potentially dangerous situations in a driving scenario. The results of this experiment showed that measures of motion perception are better predictors of performance on The Hazard Perception Test than measures of visual acuity, a measurement that is often used to assess vision for driving.
One of our lab’s research interests is investigating vision in people with migraine. Migraine is a common and debilitating primary headache disorder affecting ~15% of the general population. People with migraine can experience visual symptoms during an attack (e.g. blurred vision, visual aura) and may present to eyecare practitioners like optometrists for an eye examination. People with migraine may also attend for routine eye examinations for reasons unrelated to their migraine attacks. Because of the likelihood of seeing a person with migraine in eyecare practice, it is important for clinicians to understand how migraine might impact on vision and ocular health.
Our research, and the research of others, has shown that in between migraine attacks there may be evidence of visual dysfunction. Sometimes this visual dysfunction looks very similar to what is seen in ocular disease (e.g. glaucoma, a progressive degeneration of the optic nerve that is more prevalent with older age), except that it occurs in young people who are otherwise healthy. Migraine is a potential risk factor for glaucoma (especially “normal tension glaucoma”), so it is of interest to clinicians to consider how migraine might complicate the results and interpretation of common clinical tests that we use to diagnose and manage ocular disease, such as imaging.
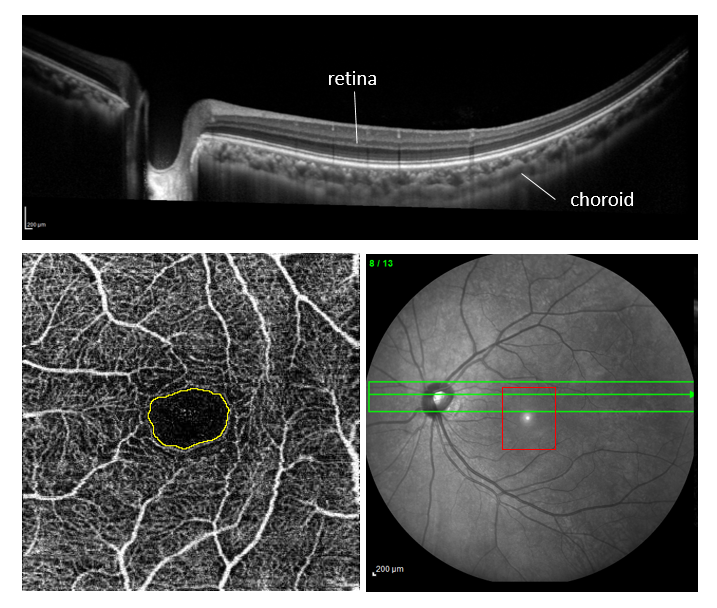
We were therefore invited to write a narrative review of the latest ophthalmic imaging evidence that the retina (at the back of the eye) may be altered in people with migraine. In the past decade, there has been considerable interest in using optical coherence tomography (OCT) to image the retina and associated structures in people with migraine. OCT is a useful device as it provides very high resolution “cross-sections” through the back of the eye, enabling us to view the individual layers of the retina and underlying vascular tissue (the choroid). More recently, OCT has advanced to enable images of blood vessels that are filled with blood (perfused vessels). Example of OCT images are shown below.
Example images of the back of the eye. TOP: OCT cross-section shows the layers of the retina and the underlying vascular tissue (choroid). BOTTOM LEFT: OCT angiography can show the central area where there are no blood vessels (foveal avascular zone) delineated by the yellow, and the network of small blood vessels surrounding the fovea. BOTTOM RIGHT: A front-on (en-face) image of the retina, indicating where the cross-section (green arrowed horizontal line) and the OCT angiography (red square) images were captured from.
Altogether, the literature published to date suggests subtle differences in retinal structure and vasculature in people with migraine. It is still too early to know whether these observations have impact later in life, as there are no longitudinal studies of retinal imaging in people with migraine. Ophthalmic imaging continues to evolve rapidly, so a key issue that future studies must consider is how to incorporate standardised imaging and analysis protocols so that people can be followed over time with the same, and hopefully not obsolete, technology.
The review paper has been published in Clinical and Experimental Optometry and can be accessed here. If you do not have institutional access, please contact us for a copy of the paper.
Neuroplasticity is the brain’s ability to change in response to the environment. Neuroplasticity is interesting to study in the context of healthy ageing, as it tells us how and why ‘you can teach an old dog new tricks’. In our lab, we are interested in a specific form of plasticity – visual neuroplasticity following temporary occlusion of one eye.
In very young animals and humans, temporarily covering one eye can lead to lifelong, irreversible reduced vision in the deprived eye. On the other hand, unlike in early life, depriving one eye for a couple of hours in adults with normal vision temporarily shifts ocular dominance to favour the deprived eye i.e. the deprived eye becomes more dominant. This counterintuitive but robust finding has been extensively studied in younger adults, but none have considered whether the phenomenon still exists in older adults.
To compare ocular dominance before and after temporary occlusion, we use a popular vision task called binocular rivalry. When the two eyes are shown two different images (e.g. the red and green striped circles below), the brain has to alternate between two percepts, and sometimes even ‘sees’ a mixed percept of the two images (e.g. overlapping red and green). Because we can measure how long each percept is seen, we can determine which eye is more dominant before patching, and then determine whether the relative dominance changes after patching. In the example below, it is typical for the two main percepts to be roughly equal before patching (or slightly biased towards one eye). After patching the ‘green’ eye for 2 hours, the green percept becomes more dominant.
Using this binocular paradigm, we show that plasticity in older adults is present and just as strong as in younger adults. This shows that the older adult visual system is able to rapidly adjust to changes in visual input when one eye is temporarily occluded, suggesting that neuroplasticity is maintained across a lifespan.
This work has been published in the neuroscience journal Cortex and the article is available here. Please contact us if you do not have institutional access.
During an eye examination, the most commonly performed clinical assessments of vision include visual acuity (the smallest line of letters that can be seen on a chart), contrast sensitivity (the minimum contrast of a letter/stripy pattern to detect it against a uniform background) and perimetry (determines the sensitivity of targets appearing in different locations in a person’s field of view). These routine clinical assessments are typically performed on plain backgrounds. However, the visual scene is more complicated in daily life and requires objects to be disambiguated from more complex visual scenes. Previous work in our lab has shown that viewing an object of interest presented on a non-uniform background can reveal interesting differences in performance, that are not tested clinically.
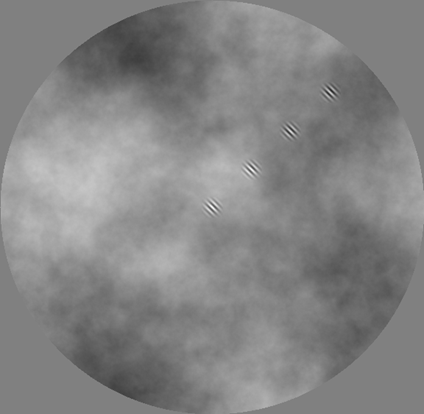
In our latest publication, we explored whether contrast sensitivity in older adults differs from that of younger adults when measured on a non-uniform background whose spatial frequency content is similar to those present in the natural visual environments. We tested 20 younger and 20 older healthy controls using a stimulus similar to that shown in the figure below.
We developed a 1/f noise background like that shown here. The oblique stripy pattern was the object of interest and was presented at four locations on the 1/f noise background (each being shown one at a time during the actual experiment).
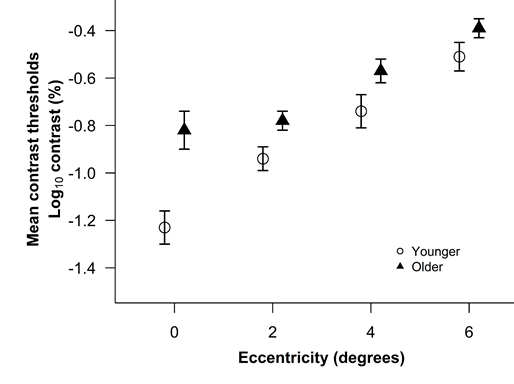
Our findings show that contrast thresholds were elevated with age with the largest difference in the thresholds between younger and older adults at the fovea compared to other eccentricities. The study findings imply that older adults have relatively greater impairment in detecting objects on non-uniform backgrounds when presented foveally than in near-foveal regions. The findings suggest that surround interactions (such as lateral centre-surround suppression) differ between older and younger adults in an eccentricity dependent fashion. This outcome may have significant implications for object perception in natural scenes for older adults.
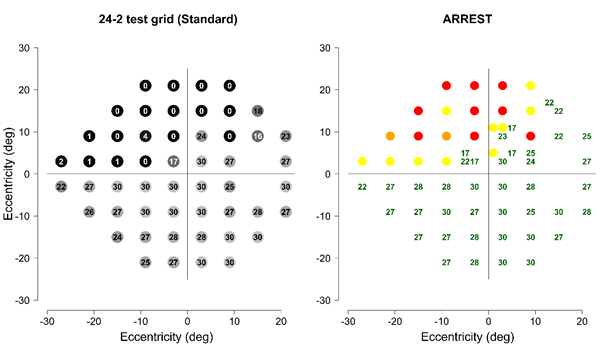
Assessing vision across the visual field (typically known as automated perimetry) is important for diagnosis and management of various ocular and neurological diseases causing progressive vision loss. Clinically used methods usually test 52 to 60 locations in the visual field and each visual field test takes approximately 5 to 9 minutes per eye, and has several well-documented limitations. Our new testing approach, the Australian Reduced Range Extended Spatial Test (ARREST) was designed to improve upon several limitations with current clinically used perimetric methods including spatial sampling (number of visual field locations tested) of the damaged visual field.
Left panel shows clinically used standard 24-2 visual field test report of a study participant with superior field loss. Right panel shows ARREST visual field report of same participant with additional test locations in the macular and in the supero-temporal field. Green represents the locations with > = 17 dB, yellow represents 0 to 16 dB, orange represents the locations classified as 0 dB, and red represents the locations classified as < 0 dB and will not be tested in the future.
A previous computer simulation study from our laboratory has shown that ARREST can improve the spatial sampling of damaged visual fields without increasing test duration with the extent of the spatial improvements depending upon the individual’s degree of visual field loss. In this research, we empirically evaluated the performance of ARREST in people diagnosed with varying severity of visual field loss. Our results support previous computer simulations that ARREST progressively improves spatial sampling of visual fields without increasing test duration. This new approach can be added to any available perimetric methods, and the parameters of ARREST can be re-engineered for disease specific requirements.
Masters of Philosophy student and Doctor of Optometry graduate, Sena Gocuk, has recently completed a project investigating the optometric care of people with age-related macular degeneration (AMD). Her project was co-supervised between the Anterior Eye, Clinical Trials and Research Translation Unit at the Department of Optometry & Vision Sciences, and the CPU Lab. Please see below for a summary of her latest publication.
Age-related macular degeneration (AMD) is a leading cause of vision impairment worldwide. Currently, there are no approved therapies for earlier stages of AMD. Treatments available for later stages of the disease may not reverse vision loss. The early identification and management of modifiable risk factors, may contribute to reducing patients’ risk of progression to sight-threatening late-stage AMD. Optometrists in Australia have a key role in providing primary eye care to people who are at risk of developing, or who have earlier stages of, AMD. They are therefore ideally placed to ask and counsel their patients about lifestyle modifications that can reduce the risk of disease progression.
Simulation of the effect of late-stage AMD on vision (1st panel: normal vision; 2nd and 3rd panel: late-stage AMD)
There are currently no studies assessing the optometric clinical care provided to patients with AMD. Self-reported surveys provide some insight however, due to their self-reported nature, there are several potential biases associated. The Macular Degeneration Clinical Care Audit Tool (MaD-CCAT), was recently developed by A/Prof Laura Downie, designed to audit the optometric care provided to people with AMD, relative to current best-practice standards. In this study, Master of Philosophy student, Sena Ayse Gocuk (who worked with Laura and Allison McKendrick from the CPULab), investigated whether performing clinical audit and receiving analytical performance feedback provides insight into current optometric clinical care and altered documentation of the care provided by optometrists to people with, or at risk of, AMD.
In her recently published article in Ophthalmic and Physiological Optics, Sena reports the findings of current optometric AMD care and improvements in clinical record documentation of key aspects of clinical care including AMD risk factors, clinical examination, AMD severity classification, and management advice.
Her findings support a role for audit, to improve optometric clinical care of AMD, as evidenced by improved documentation of the AMD care delivered.
Poorly illuminated roads lit only by car headlights are commonly experienced by many nighttime drivers. This type of lighting condition is called “mesopic”, and the visual system operates differently under these conditions relative to daylight conditions. Humans have two types of visual photoreceptors (rods and cones) in the retina. In bright light, only cones contribute to vision. But under mesopic conditions, both types of photoreceptors work together. There are differences in the timing of responses from these two types of photoreceptors, and differences in their neural circuitry, which makes mesopic visual experience differ from that during daylight.
A poorly illuminated road at The Grampians, Victoria, Australia
There is still a lot that we do not know about the precise changes to vision under mesopic conditions. To address this gap, PhD student Juan Sepulveda, has recently conducted a study investigating the perception of various types of moving objects observed in low light level conditions. In his recently published paper in Ophthalmic & Physiological Optics, he reports the findings of these experiments, which importantly also consider the effects of age and location of the stimuli in the visual field. He found that for most of the stimuli tested, older adults have poorer performance under daylight viewing conditions compared to younger adults. Dimmer lighting conditions impacted the perception of motion to similar extents in both age groups (both groups had worse performance). Because older adults already have reduced ability to perceive some moving stimuli in daylight, the additional decrement in performance caused by dim light resulted in even more severe deficits in performance in some individuals. These findings may have potential implications in everyday tasks such as nighttime driving situations.
Juan testing biological motion perception
Results of the motion tasks in light (white panels) and dim (violet panels) conditions
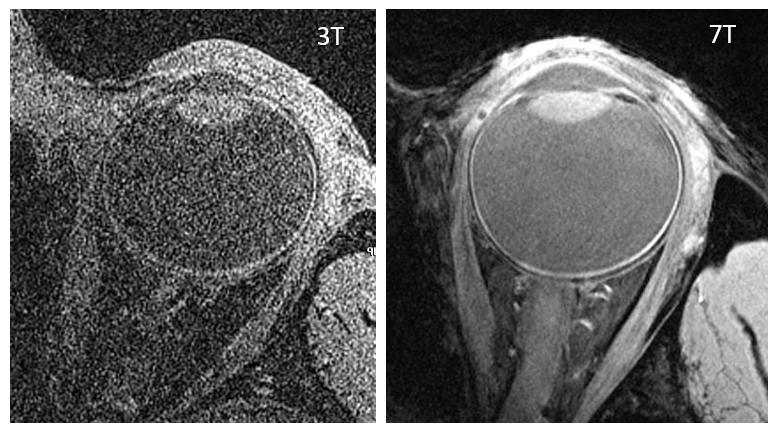
Thanks to a Melbourne Neuroscience Institute fellowship, Dr Bao Nguyen was able to spend a year pursuing a new collaboration between our lab and the Melbourne Brain Centre Imaging Unit at the University of Melbourne. The Imaging Unit houses a unique combination of a state-of-the-art 7 Tesla magnetic resonance imaging scanner (known as 7T MRI, which has improved signal-to-noise ratio compared with conventional clinical scanners of 1.5T and 3T) and a dedicated eye coil (not the usual head coil that is used for brain imaging) that is designed specifically for imaging the eye and surrounding anatomy.
Our collaboration has led to two papers. Firstly, we were invited to feature our work in a special issue of Magnetic Resonance Imaging Clinics of North America describing how we used the technology to acquire 2D and 3D images of ocular anatomy. We demonstrated that, with careful consideration of participant preparation and sequence selection to maximise image quality, it is clinically feasible to obtain ultra high field ocular and orbital MRI images with minimal artefacts. This information is useful for improved MRI investigations of ocular conditions that affect the structural integrity of the eye and its surrounding anatomy. The paper can be accessed here.
Example 3D MRI images (0.2 x 0.2 x 0.4 mm size, 44 slices) at 3T with a 64 channel head coil (left) versus at 7T with a 6 channel eye coil (right)
Our second paper, published in Translational Vision Science and Technology, demonstrates the feasibility of using 7T MR-EYE (with a dedicated eye coil) to enable measurement of the optic nerve, subarachnoid space (where fluid surrounding the brain also flows) and optic nerve sheath (the protective covering around optic nerve) behind the eye. The area just behind the eyeball, where the optic nerve exits the eye, is of clinical interest because this is where changes in intracranial (brain) pressure can impact on the optic nerve. It is also of clinical interest to better understand why some optic nerves may be more susceptible to damage, such as in eyes that are elongated (high short-sightedness, or myopia). Because one of the major advantages of MRI over conventional ophthalmic imaging such as optical coherence tomography (OCT) is the ability to image anatomy at depths behind the eyeball, we used our MR-EYE technology to image young, healthy eyes with and without high myopia to see if there were any anatomical differences. Our findings suggest that even without any signs of optic nerve damage, the cross-sectional dimensions of the optic nerve and fluid-filled subarachnoid space behind the eyeball are influenced by the degree of myopia. The paper is available to read open-access here.
7T MR-EYE can be used to take a ‘slice’ (see green line) through the optic nerve about 3mm behind the eyeball. The cross-sectional slice obtained can then be imaged to measure the cross-sectional area of the optic nerve, surrounding fluid-filled subarachnoid space, and surrounding optic nerve sheath
Part of this work has also been presented at several national and international conferences, including at the 2019 Association for Research in Vision and Ophthalmology in Vancouver, Canada (in the pre-COVID era!)
Dr Bao Nguyen presenting her MR-EYE poster at the 2019 Association for Research in Vision and Ophthalmology in Vancouver, Canada
Often we assume that with ageing that physical and sensory processing slows. However, this is not always the case. Our lab has been interested in a visual phenomenon called ‘centre-surround contrast suppression’ for several years. This phenomenon describes a general effect whereby the perceived contrast of an object does not just depend on its physical contrast, but also on the features of its background. As a specific example, if an object is actually 40% contrast, when you place it within a surround of higher contrast, the perceived contrast may be substantially reduced (e.g. appears 20% or looks much “greyer” than when presented on its own). This is a powerful demonstration of perceptual surround suppression.
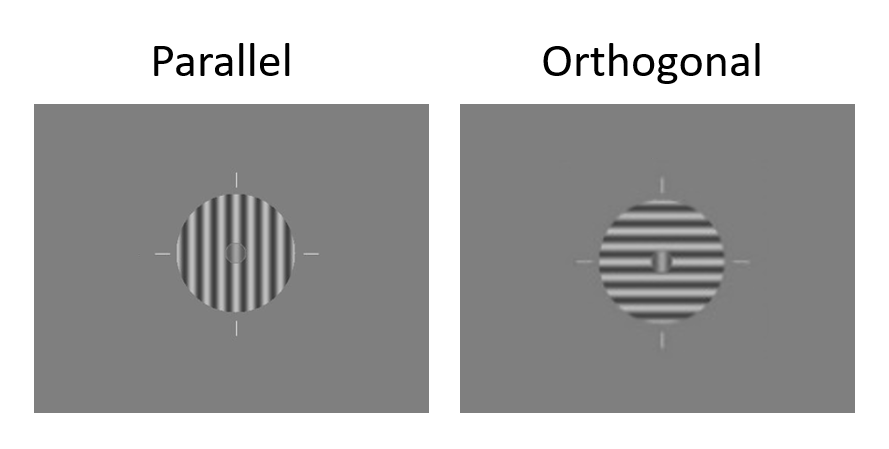
Perceptual surround suppression is stronger when the centre and surround have the same orientation (parallel) compared to when the centre and surround orientation are 90 degrees different from each other. Examples of parallel and orthogonal centre-surround visual stimuli are shown below.
On the left is a parallel centre-surround stimulus, where the stripes are oriented the same way (vertical). On the right is an orthogonal centre-surround stimulus, where the centre comprises vertical stripes and the surround comprises horizontal stripes.
Previous studies, from our lab and others, have shown that older and younger adults can differ in the strength of perceptual surround suppression effects.
In our new publication, we used scalp electrodes to non-invasively measure the electrical signals from the brain using electroencephalography when people viewed these centre-surround stimuli. Older and younger adult brains decoded orientation information (i.e. differentiated between parallel and orthogonal centre-surround stimuli) at the same time after the stimulus appeared. That is, there does not seem to be a deleterious effect of ageing in the ability to accumulate visual information to make a decision about the appearance of these patterns – older people seem to accumulate sufficient sensory information at the same time as younger adults to be able to distinguish between parallel and orthogonal centre-surround stimuli.














{kind=link}